Authored by Aziz VM
Abstract
In this paper we aimed at looking at the renal profile and its impact on cognition. The research aims to test the renal profile of patients with dementia or delirium as part of the physical health care check and to review its effect on cognition. We looked at renal profile for all patients admitted to a psychiatric unit with a diagnosis of dementia and compared them with patients diagnosed with delirium/ dementia who were referred to the psychiatric liaison team within 6 months period.Seventy-six patients suffering dementia were admitted to a Psychiatric Unit and sixty-one suffering delirium/ dementia seen by Liaison Psychiatry Services in District General Hospitals (DGH) were sampled (Total 137 patients). The mean age of the sample was 80.85 years old (SD = 8.32) and 56.9% were females (n = 78). Vascular risk factors were present in 79% of dementia patients in the psychiatric unit (n=60) versus 83.6% of Liaison psychiatry patients (n= 51). CT head scan were done on 129 patients (94%), and 69% (n= 89) of the scans showed vascular brain insult. Multivariate analysis yielded no significant association between both the diagnosis and the presence of vascular risk factors in both groups and the renal profile.
Our paper highlighted the need to ensure that cognitive testing and brain scans are completed for all patients as much as possible. Both Mental Health Services and District General Hospitals are to consider implementing a dementia-physical health pathway to improve the physical health of patients with cognitive impairment. Comparing the Renal Profile of patients with Dementia admitted to a Psychiatric Unit to those with Delirium/ Dementia seen by the Liaison Psychiatric Services in District General Hospital (DGH) in Wales.
Keywords: Renal; Profile; Impairment; Dementia; Delirium; Vascular; Cognitive
Introduction
Physiological functions, including kidney function, are strongly associated with age. Glomerular filtration rate (GFR), which is a marker of chronic kidney disease (CKD), declines with age in healthy adults [1]. CKD is defined as a condition with an estimated GFR (eGFR) of less than 60 mL/min per 1.73 m2 or continuous presence of kidney impairment (e.g., albuminuria) for 3 months or longer [2].The Hisayama Study Group has investigated the relationship between CKD and vascular risk and reported that the former was an important risk factor for cardiovascular disease [3] and that people with metabolic syndrome had a higher incidence of CKD [4]. CKD has also been established as an independent risk factor for cerebrovascular disease (CVD) and cardiovascular disease [5,6]. One study [5] reported that, in middle-aged community-based adults, the combination of CKD and anaemia was associated with a substantially greater risk of stroke independent of other known risk factors for stroke.
The prevalence of CKD has been shown to be higher in older adults in Japan [7] and internationally [8]. Approximately 20% of the Japanese adult population is estimated to have Stage 3 to 5 CKD, which represents kidney impairment [7]. Recent studies have shown impaired kidney function to be associated with greater prevalence of cognitive impairment [9,10] a more-rapid rate of cognitive decline [11], and incident cognitive impairment [12-14]. Three studies reported associations between kidney function and cognitive impairment at an eGFR threshold of less than 60 mL/min per 1.73 m11,13 a fourth reported that the threshold effect was at a lower GFR (eGFR<45 mL/min per 1.73 m2) [14]. and a fifth reported the threshold effect to be at a much lower GFR (eGFR<30 mL/min per 1.73 m2) [10]. All studies reported age, hypertension, and diabetes mellitus to be independent factors in the association between kidney function and cognition, but an association between CKD and dementia onset has not been reported, with the exception of one study [12], which used serum creatinine but not eGFR for assessment of kidney function.
In this research we aimed at looking at the renal profile and its impact on cognition. The paper aims to test the renal profile of patients with dementia or delirium as part of the physical health care check and to review its effect on cognition.
Methodology
Our design was a combined cross sectional and prospective data analysis. We looked at renal profile for all patients admitted to a psychiatric unit with a diagnosis of dementia and compared them with patients diagnosed with delirium/ dementia who were referred to the psychiatric liaison team within a 6 months’ period.A clinical team consisting of an inpatient consultant psychiatrist, a liaison consultant psychiatrist and higher trainee registrar reviewed the medical records, ensured the renal profile was completed, and did cognitive assessment using either he Addenbrooke’s Cognitive Examination-III (ACE-III) which is a brief cognitive test that assesses five cognitive domains: attention, memory, verbal fluency, language and visuospatial abilities; or Montreal Cognitive Assessment (MoCA) together with reviewing the brain scans where indicated. The patient’s diagnosis, medical history, co-morbidities and medications were also noted together with any relevant demographic data. The vascular risk factors such as CKD, hypertension, dyslipidaemia, diabetes mellitus, IHD, and anaemia were noted.
Result
Demographics (Table 1)
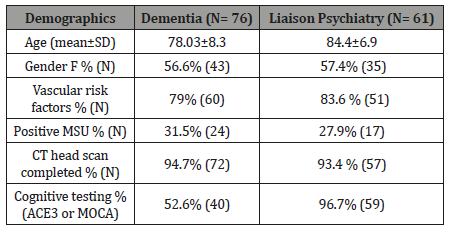
Seventy-six patients suffering dementia were admitted to a Psychiatric Unit and sixty-one suffering delirium/ dementia seen by Liaison Psychiatry Services in District General Hospitals (DGH) were sampled (Total 137 patients). The mean age of the sample was 80.85 years old (SD = 8.32) and 56.9% were females (n = 78). Vascular risk factors were present in 79% of dementia patients in the psychiatric unit (n=60) versus 83.6% of Liaison psychiatry patients (n= 51).31.5% (n= 24) of patients in the psychiatric unit while 27.9% (n=17) of DGH patients had positive MSU with E-Coli, E Faecalis, Proteus or mixed heavy growth. Females were associated with more urine infections than males, X2 (1, N = 76) = 10.316, p =.001. Odd ratio (OR) for females = 0.44 vs. OR for males = 0.18. CT head scans were done in 129 patients (94%), and 69% (n= 89) of the scans showed vascular brain insult. Cognitive testing was done in 40 patients with dementia in the psychiatric ward (52.6% ACE3 or MOCA) and 59 patients with delirium/ dementia in the DGH (96.7% had MOCA). The mean number of comorbidities per individual was 4 items (SD±2.03). While the mean number of medications was 10.3 items (SD±4, range 4-18) (Table 1).
Table 1: Demographics.
Diagnosis
Vascular dementia and Alzheimer’s constituted the majority of diagnoses (72.3%). Alzheimer’s disease (37.2%, n = 51), Vascular dementia (35%, n= 48), mixed dementia (11%, n= 15), Lewy Body dementia (5%), and other diagnoses included Parkinson’s disease, Alcohol-related brain damage, Frontotemporal dementia, and Dementia NOS, and in six patients the primary diagnosis was delirium (in the DGH).
Co-morbidities
Hypercholesterolemia, Hypertension, AF, COPD, Osteoarthritis, Macular degeneration , Myocardial infarction, IDDM, CKD, Breast cancer, Uterine cancer, Stoke, DVT, Type 2 Diabetes Mellitus, Recurrent UTIs, Inguinal hernia, Heavy smoking, DVT, Ischaemic heart disease, Hypothyroidism, TIA, Parkinson’s disease, Angina, Asthma, Epilepsy, Rectal cancer, Arthritis, Alcohol excess, Myasthenia gravis, OA Knees, CCF, Pernicious anaemia, Hiatus hernia, Vertigo, Osteoporosis, Carotid artery disease, Hip fractures, Cervical spondylosis, Constipation, rheumatic fever, systematic focal epilepsy, Lung cancer, spondylosis, hysterectomy, Inguinal hernia, osteoarthritis, Grand mal seizures, Duodenal ulcer, Diverticulitis, CVA, Hydronephrosis, impaired glucose tolerance, cataracts, Retinal detachment, Colon cancer/subtotal colectomy, lower urinary tract symptoms, fractured neck of femur, Prostate cancer, spinal stenosis, reflux oesophagitis, varicose veins.Archoidosis, Kidney disease, DVT/PE, Urinary retention, Haemorrhoids, Myoclonic jerks, Progressive supranuclear palsy, overactive bladder, benign prostatic hypertrophy, Knee surgery, Depression, Chronic Kidney Disease, Viral encephalitis, haematuria, bilateral leg oedema, pressure sores , thyrotoxicosis and sepsis, chronic back pain, renal calculi, left posterior vitreous reattachment, hypotension, cholecystectomy, chronic kidney disease stage 4, IBS, anxiety, spondylitis, palpitations , acquired brain injury secondary car accident, Pseudo gout, Falls, Cholecystectomy, fractured wrist, SDH, Non-toxic multinodular goiter (Table 2).
To read more about this article....Open access Journal of of Biomedical Engineering & Biotechnology
Please follow the URL to access more information about this article
https://irispublishers.com/abeb/fulltext/comparing-the-renal-profile-of-patients-with-dementia-admitted-to-a-psychiatric-unit-to-those-with-delirium-dementia.ID.000523.php
To know about Open Access Publishers




No comments:
Post a Comment